
On October 29, Smith & Nephew, the venerable 159-year-old supplier of orthopedic implants and instruments, agreed to plunk down $275 million to buy one of the fastest growing young robotics companies in medicine—12-year-old Blue Belt Holdings, Inc.
In the last 12 months Blue Belt has sold 40 of its Navio systems and close to 2, 000 partial knee replacement surgeries have been performed using the Navio.
Two years ago (November 2013) Stryker Corporation bought MAKO Surgical, the largest and most successful supplier of robotic devices for orthopedic surgery, for $1.65 billion.
Smith & Nephew paid slightly more to acquire Blue Belt (14x sales) than Stryker did to buy MAKO (13x) but Stryker’s commitment (6% of its market capitalization) was larger.

Robotics – Transforming Orthopedics
The Harvard Business Review called surgical robots one of “10 Innovations That Will Transform Medicine.” In 2012, Global Analysts, Inc. predicted that worldwide demand for service robots (which includes medical) would eventually reach $38.42 billion. Now two major orthopedic companies—Stryker and Smith & Nephew—have put a collective $2 billion bet on robots.
Douglas Padgett, M.D., chief of Adult Reconstruction for Hospital for Special Surgery in New York, uses robotic assist devices and says; “Surgical navigation is not enough [of a benefit]. These robotic assist systems improve both the precision and the accuracy of each case which reduces, for example, problems associated with poor socket placement. With the system any surgeon can improve the accuracy of their bone preparation as well as the precision of their implant delivery.”
Robotics, as a tool to standardize precision in surgery, are a very big deal.
50% of all Hip Procedures Imprecise
In a study of 2, 061 total hip revisions, researchers found that 50% of the acetabular cups were outside the optimal range in terms of both version and abduction. The study, which won the John Charnley Award, and published in the journal Clinical Orthopedics and Related Research (Orthop Relat Res. 2011 Feb;469(2):319-29), looked at postoperative AP pelvis and cross-table lateral radiographs on patient who received a total hip arthroplasty or hip resurfacing from 2004-2008.
From 1, 823 hips, 1, 144 (63%) of the acetabular cups were within the abduction range (defined as movement of a limb toward the midline or axis of the body) and 1, 441 (79%) were within the version range (defined as the tipping angle of the joint) but ONLY 917 (50%) were within the range for both.
Why so poor? The authors (Callanan MC, Jarrett B, Bragdon CR, Zurakowski D, Rubash HE, Freiberg AA, Malchau H.) said that surgical approach, surgeon volume and obesity independently predicted mal-positioned cups.
Surgical-assist tools like Blue Belt’s Navio or MAKO’s Rio address two of the three factors which, according to the study, affect malpositioned cups.
Approximately 280, 000 total hip replacement procedures are performed in the U.S. annually. That number implies that between 2004 and 2008 (the study period) roughly 700, 000 patients received mal-positioned artificial hips and are at risk for instability, lysis and revision surgery.
The Consequences of Mal-Positioning
Mal-positioned knee or hip components are by far the most common cause of poor outcomes and revision surgeries. In the case of hips, two bad things happen when the cup or stem is mal-positioned: the ball starts to rattle around inside cup and may come out entirely (instability) or the two components start rubbing together unnaturally and tiny particles of either component break off and cause inflammation (lysis).
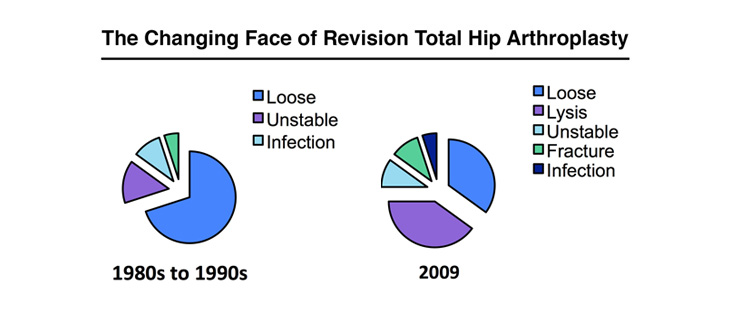
In the last 10 years instability and lysis have become the dominant causes of hip failure.
And the cost of correcting or living with mal-positioned knees or hips is, conservatively, billions of dollars. By contrast, the cost of pursuing perfection using surgical robots may well be just hundreds of millions of dollars.
Robotics: Medicare’s Friend
In July 2015 Medicare introduced a revolutionary five-year bundled payment model, called the “Comprehensive Care for Joint Replacement (CCJR) Program” which will pay 750 hospitals in 75 geographic areas a lump sum for each hip and knee replacement episode starting from hospital admission to 90 days after discharge. At the end of a year, those hospitals will have a chance to earn more money or have some of their payments clawed back by Medicare, depending on patient outcomes.
In September 2015 the 500, 000 member Colorado Public Employees Retirement Association offered its members the opportunity to receive their hip or knee replacements for a fixed cost, all in.
Robotics, it seems, may become one of the tools that will help hospitals to participate in the coming flat fee, bundled care large joint future.
Robotic assisted surgery addresses the 82% of the cost of knee or hip reconstructive surgery that is non-implant related. These are the surgeon, anesthesia, nurses, rehab and poor outcomes or revision costs.
Small gains—like fewer errors, more consistent outcomes, less blood loss, more efficient surgeries—can have a huge effect on overall costs.
Not surprisingly, surgical robots have had the greatest acceptance in the most technically challenging procedures like neurosurgery (first used in the 1980s), oral and maxillofacial surgery (extremely tight tolerances), laparoscopic abdominal or gynecological surgery, cardiac surgery and uni-knee replacement procedures.
How Do Surgical Assist Devices (Robots) Work?
Surgical robots use computer technology to accomplish two things—improve pre-surgery planning and, in collaboration with the surgeon, perform a more accurate and precise surgery which, in turn, improves long term outcomes.
The whole process starts with an accurate model of the patient’s anatomy. A typical system creates a 3D dimensional data set which is an exact geometrical map of normal and pathological tissues and structures at the operative site. Typically, CT is preferred. MRI data sets can have volumetric deformations.
Then these systems analyze and process the image data. One trick programmers have built into these systems is to color contrast different anatomical levels so that hard structures like bone are easy to distinguish from soft tissues like cartilage or arteries and veins.
Using the virtual 3D anatomical model, surgeons refine their diagnosis and simulate the upcoming surgery. When all surgical planning is done, the robot then uses that data to program pre-planned actions during actual surgery.
During surgery, the robot (or surgical assist device) uses these programmed images and surgeon-generated datasets to direct the actual surgery.
There are three basic types of surgical robots:
- Supervisory controlled – robot executes a series of pre-programmed actions and actually performs the surgery.
- Telesurgical – also known as remote surgery, the surgeon manipulates the robotic arms during the procedure.
- Shared-control – the surgeon performs the surgery and the robot uses the pre-programmed information to provide steady-hand manipulations of the instrument.
Both Blue Belt and MAKO’s systems are shared-control systems. The surgeon directs the cuts and burrs, but the robot makes sure that every move is precise according to the patient’s own anatomy.
Economic Rationale
The #1 hurdle to adoption for any robotic assist system is cost. MAKO’s systems run about $1 million with an annual fee of about $100, 000. Blue Belt’s systems cost about $400, 000 with an annual fee of about $40, 000.
So, what is the economic rationale for these systems? There are three basic arguments:
- The cost of precision must be less than the cost of imprecision.
- The robot must deliver consistently excellent outcomes.
- The robot must be a platform technology that can be employed for multiple indications. After it is fired up at 6am, it must be able to be used continuously until the last patient is wheeled into recovery. In a medium size orthopedic practice this probably means a platform for knee, hip, shoulder, elbow, hand or any other surgery so that the cost will be amortized over the maximum number of surgeries. In a high volume large joint practice, it means knees and hips.
Wall Street’s Take
Two billion dollars is a lot to pay for these two young firms—12-year-old Blue Belt or 9-year-old MAKO.
But surgical robotics companies operate in a different Wall Street universe than implant suppliers.
Intuitive Surgical, Inc., the pioneer for surgical robotic assist systems and supplier of the da Vinci Surgical System robot is now 20 years old and Wall Street’s investors have afforded the company a $18.64 billion market value.
Investors think Intuitive’s sales are worth about $8 for every $1 generated. By contrast, investors think that Smith & Nephew’s sales are worth $3 for every $1 generated and Stryker’s sales are worth about $4 for every $1 generated.
Wall Street puts a much higher value on surgical robotics than on implant suppliers.
How Will Blue Belt and Smith & Nephew Do?
In its SEC filings, Smith & Nephew said “We expect annual revenue growth at Blue Belt Technologies to be in excess of 50% over the medium-term from a 2015 base of approximately $19 million. Investment in the combined R&D programmes and supportive clinical evidence will dilute Group trading profit margin by around 60bps in 2016, with the business becoming profitable in 2018. Return on capital employed is expected to exceed our weighted average cost of capital in year four.”
In addition, Smith & Nephew plans to roll out the Navio robotics system for its JOURNEY UNI partial knee and the recently acquired ZUK uni knee.
In 2017, SNN hopes to be able to launch a total knee Navio system to support the JOURNEY II as well as SNN revision knee systems and the JOURNEY II XR bi-cruciate retaining knee arthroplasty system.
Last week Stryker reported its results for the first six months of 2015 and MAKO, which it had purchased about two years ago, announced that it had placed 13 robots in the second quarter, up from 9 in the first quarter.
If Stryker’s experience is any clue, Smith and Nephew should do well with Blue Belt.
Robotic assisted surgery is well on its way to becoming part of the orthopedic standard of care.
